

Normal Renal Function

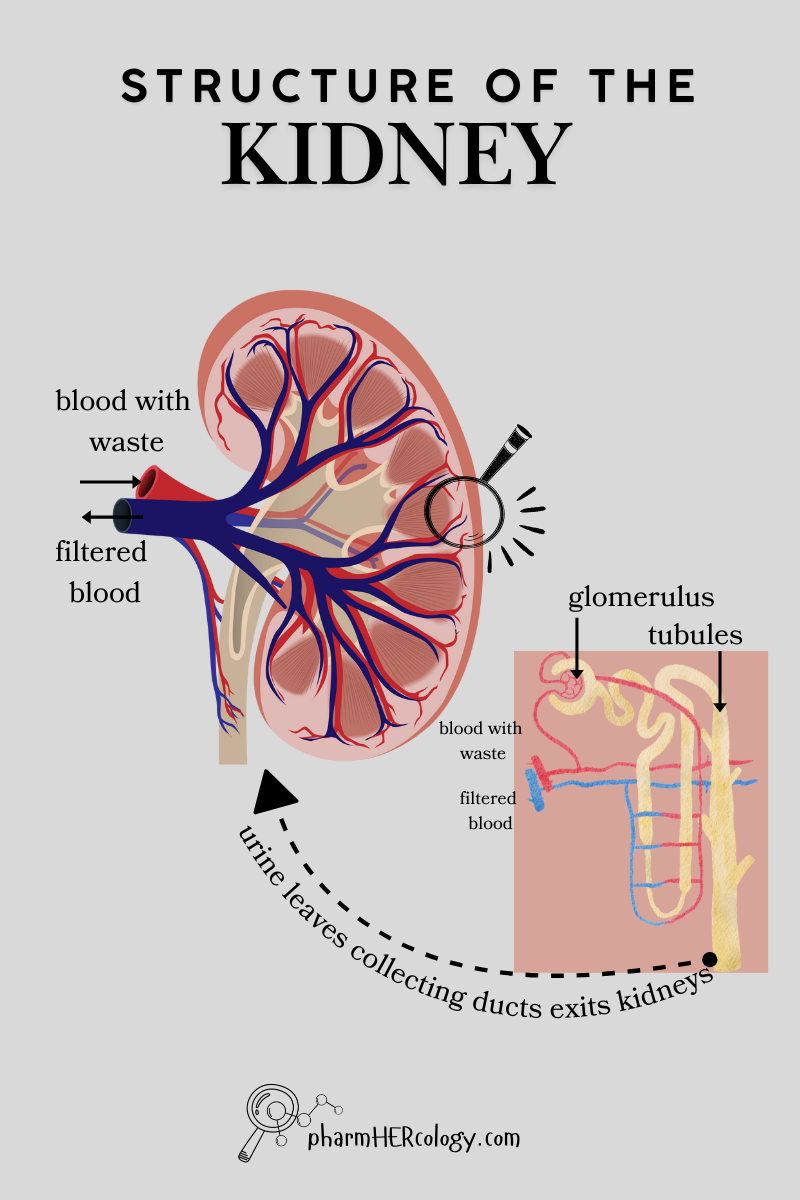
The kidneys has many roles including filtration of blood to remove waste.
Within the kidneys waste is filtered at the glomerulus. Waste exists the kidneys via the tubules as urine. Filtered blood is returned to the body.
Categories of Renal Injury
There are three broad categories of renal injury based on where dysfunction occurs.

Prerenal: dysfunction in parts prior to the kidneys that affect renal processes
Intrinsic: injury within the kidneys
Post Renal: Injury beyond the kidneys that affect renal processes
There are 5 markers that we use to distinguish between these categories of acute renal injury.
- The ratio of BUN to creatinine in plasma
- The concentration of sodium in the urine
- The fractional excretion of sodium
- The fractional excretion of urea
- The type of sedimentation in urine

BUN/SCr Ratio

BUN and creatinine used for this calculation are both measured in plasma. Both are cleared by the kidneys at the glomerulus. The glomerulus is the cluster of blood vessels inside the kidneys where filtration occurs.
{kind=link}
Prerenal
Filtration by the glomerulus depends on the difference in pressure of plasma entering and plasma leaving. Any disruption to blood flow entering the kidneys will decrease filtration. Prerenal dysfunction refers to this hypoperfusion at the glomerulus.
The cause of hypoperfusion may is isolated to the kidneys or could be systemic. As the rate of clearance slows down waste products accumulate leading to increases in both urea and creatinine.
They increase at different rates with urea accumulating faster. Therefore we see an overall increase in the ratio of the two values.
Intrinsic
When there is internal damage to the kidneys, the filtration system is damaged. You can think of it as being leaky.
More plasma solutes, including urea and creatinine move through the glomerulus resulting in lower plasma concentrations. Which means the ratio of BUN to Scr is lower than normal.
Post Renal
Post renal kidney injury is most often bladder outlet obstruction. An obstruction to the outflow of urine increases pressure at the glomerulus. This damages the sensitive vessels leading to intrinsic damage.
Because of this, post renal injury often looks like intrinsic. It is classified differently because it originates outside of the kidneys.
The increased leakiness caused by the pressure of obstruction increases plasma clearance of urea and creatinine with a corresponding decrease in the BUN/Scr ratio.
Subscribe for Access to Exclusive Content
Urinary Sodium

Urinary sodium (UNa) measures sodium concentration in a spot urine sample. The concentration of sodium in urine is usually around 20mEq/L. This is sodium that has been filtered out of blood at the glomerulus in the kidneys.
Prerenal
When there is prerenal injury, there is reduced blood flow to the kidneys which is detected by angiotensin II receptors in renal tubules. The kidneys interpret decrease in flow as a decrease in blood pressure.
To compensate it will increase reabsorption of sodium and water within the kidney tubules. This results in less sodium being filtered into urine and a corresponding decrease in urinary sodium (UNa).
Intrinsic
When there is intrinsic injury in the kidneys we expect the filtration system to be more leaky than normal and so more sodium will make it into the urine. The UNa is expected to be higher than normal.
Damage to tubules within the kidneys also means there is less reabsorption of sodium. Normally almost all sodium filtered at the glomerulus is reabsorbed by the kidneys at varies tubules.
The proximal tubule reabsorbs ~60% of sodium. The loop of Henle absorbs ~25%. The convoluted tubules and collecting ducts absorb ~10%. Therefore the degree of sodium wasting is influenced by where injury in the kidney occurs. This add to the amount of sodium in urine with intrinsic injury.
Post Renal
Post renal injury leads to intrinsic injury by increasing renal pressure we would see in increase in urinary sodium with post renal injury.
Fractional Excretion of Sodium
Fractional excretion of sodium (FeNa) is measured by obtaining a plasma sample and urine sample at the same time and testing the levels of sodium and creatinine in each sample.

Fractional excretion of sodium is the ratio of sodium in urine and plasma divided by the ratio of creatinine in urine and plasma. This is often expressed as percent (x100). It calculates the proportion that made it out of plasma and into urine.

Prerenal
When there is decreased perfusion to the glomerulus the normal filtration processes at the glomerulus and within the tubules will continue to occur. The only difference is that less sodium and less creatinine is being introduced at the glomerulus so we see a lower concentration of each in the urine.
The proportions of each in the urine and plasma will remain the same which is why the ratio does not change and FENa will appear normal even with prerenal injury.
Intrinsic
This is similar to what we saw with urinary sodium. Damage to the glomerulus results in “leaky pipes”. More sodium and creatinine is going to get through than usual.
Damage to tubules within the kidneys also means that there is going to less reabsorption of sodium. This results in a significant increase in sodium wasting.
Urinary sodium is the numerator in our FeNa equation. Its is going to have a greater increase in urinary concentration. The FENa is expected to be higher than normal with intrinsic injury.
Post Renal
Post renal calculations will mimic intrinsic calculations because the increased pressure from outlet obstruction leads to intrinsic damage. The FENa is expected to be higher than normal with post renal injury.
Fractional Excretion Urea
Fractional excretion of urea (FEU) is essentially the same as FENa except we use urea instead of sodium. It is measured by obtaining a plasma sample and urine sample at the same time and testing the levels of urea and creatinine in each sample.
Why have both? Sodium levels can be affected by alot: diuretics, chronic kidney disease, sepsis, heart failure. FENa may not be valid in those cases. The use of FEU is recommended.

Fractional excretion of urea is the ratio of urea in urine and plasma divided by the ratio of creatinine in urine and plasma. This is often expressed as percent (x100). It calculates the proportion that made it out of plasma and into urine.

Prerenal
The mechanism is similar wat we saw with FENa. When the cause of injury is prerenal the only difference will be a decrease in the amount of urea introduced at the glomerulus for filtration. All other processes beyond the glomerulus remain intact.
The proportions of urea and creatinine in the urine and plasma will remain the same which is why the ratio does not change and FEU will appear normal even with prerenal injury.
Intrinsic
Damage to the glomerulus will cause more urea to leak through increasing the concentration of urea in urine. Urea is also “recycled” multiple times in the collecting ducts of the tubules before it is excreted into urine. Damage to the collecting duct will result in less recycling and more wasting, further increasing the amount of urea extracted into urine.
Post Renal
The build up in pressure caused by post renal injury can lead to intrinsic injury which is why the FEU values tend to be similar. The only difference is where the injury originated.
Urine Sedimentation
When a urinalysis is ordered, it involves the observation of urinary sediments microscopically. The sediments are derived by centrifuging the urine sample to separate solid components from the liquid. Those solid components are urine sedimentation.
Normal urine sedimentation includes low quantities of red blood cells, white blood cells and epithelial cells.

Abnormal sediments found in urine during acute renal injury are the result of dead renal tissue that sloths off and is eliminated in urine.
Prerenal
In acute prerenal dysfunction there is only decreased perfusion. All tissues within the kidneys remain in tact. Urine sedimentation remains normal.
Intrinsic
In intrinsic dysfunction there actual damage to tissues within the kidneys. Medications like aminoglycosides can absorb into the cells of the kidneys and cause necrosis. The cells die, sloth off and are eliminated in urine. Inflammation within the kidneys caused by autoimmune diseases or infection causes an influx of immune modulators that can directly damage tubules and glomeruli.
When there is damage to tissue within the kidneys muddy brown granular cast and renal epithelial cells from dead kidney cells are present on urinalysis.
Post Renal
The degree to which post renal obstruction causes intrinsic damage determines the degree of sedimentation that will be observed on urinalysis. It can range from normal to casts and epithelial cells.
I hope this unit has provided clarity on how we distinguish the 3 types of acute kidney injury based on the origin of dysfunction. Now you have a good foundation to dive into the AKI guidelines and renal supplementation strategies. If you’ve found this unit helpful I would love to hear from you. Leave a question or comment below!

Subscribe
Subscribe to get the latest study unit in your inbox.
The information on this website is intended to be used solely for educational and informational purposes. While the content may be about specific medical and health care issues, it is not a substitute for or replacement of personalized medical advice and is not intended to be used as the sole basis for making individualized medical or health-related decisions.
3 thoughts on “Renal Injury: What You Need to Know”